How long is too long? Rethinking the Huntington’s disease ‘gray area’
Does an ‘intermediate’ CAG repeat count in the Huntington’s disease gene cause brain changes?
By Dr Peter McColgan August 19, 2013 Edited by Professor Ed Wild
The Huntington’s disease genetic test involves counting the number of CAGs at the start of the HD gene. Some results are in a ‘gray area’ - larger than normal but smaller than the range that causes HD. Now, by closely studying people with CAG counts in the intermediate range, the PHAROS study has found some subtle differences in mood and behavior. These results don’t mean that intermediate CAG counts cause HD, but they do suggest they may have some effects on the brain, which need to be studied in more detail.
CAG repeats and the gray area
Our genes are made of DNA, which in turn is made up of four chemical building blocks referred to as A, C, G and T. These stand for adenine, cytosine, guanine and thymine. These chemicals form the ‘letters’ of our genetic code, which are used as instructions for making proteins – the molecular machines that do all the important stuff in our cells.

The gene that causes Huntington’s disease is called the huntingtin gene. It has an interesting stretch near the beginning, made of the letters C-A-G repeated several times. Huntington’s disease happens to people who have too many of these CAG repeats in the gene.
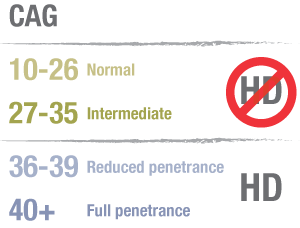
Most huntingtin genes have between 10 and 26 CAG repeats and this range never causes Huntington’s disease. But people with over 40 or more repeats in the huntingtin gene will develop Huntington’s disease at some time in their life.
In the middle – sometimes called the gray area - things get a bit more complicated. People with 36-39 CAG repeats may get Huntington’s disease or may not – it’s impossible to know for sure. If they do, their symptoms usually begin later in life. 36-39 is called the ‘reduced penetrance’ range.
The intermediate range of CAG repeats
That leaves a gap between 27 and 35 CAG repeats to deal with. This is called the ‘intermediate’ range, and it’s what this article is about. Something like 1% of people in the general population have a huntingtin gene in this intermediate range.
According to our current understanding, a CAG repeat length in the intermediate range does not cause Huntington’s disease or any of its symptoms.
Wait a minute! If the intermediate range doesn’t cause HD, how is it any different from the normal range? The difference lies in what can happen when intermediate-length genes are passed from parent to child. When this happens, there’s an increased risk that an intermediate gene will expand to have a higher CAG count that can cause HD. The exact risk of this happening is very low, however, and in most cases people with ‘intermediate range’ genes don’t have kids with disease-causing genes.
But even if that happens, the person with the intermediate CAG count will never get HD themselves.
Let’s recap
So… 26 or fewer CAG repeats is normal, while 40 or more causes HD. 36-39 CAG repeats might cause HD later in life. And the intermediate range, between 27 and 35, doesn’t cause HD but does carry a small risk of passing a larger, possibly harmful huntingtin gene to the kids.
That, at least, is our current understanding of the situation.
One slightly extreme way of putting it would be to declare: “people with intermediate CAG repeat lengths don’t have any brain differences from people with normal-length genes”.
“Do these subtle changes represent a very early stage of Huntington’s disease? That’s a very bold claim, and not one that can be proved either way at the moment. ”
But researchers are a curious bunch, and naturally wondered whether that simple statement is really true. After all, if lots of something is bad, isn’t it possible that a medium amount is a little bit bad?
The PHAROS Study
The PHAROS study stands for Prospective Huntington’s at Risk Observational Study. It involves 43 medical centres across America and includes 1001 people.
Those enrolled in the study have a parent, brother or sister with Huntington’s disease, but had not had an HD genetic test themselves until taking part in the study. PHAROS tested all its participants, but the test results were not revealed to them or the study personnel – the results were kept secret and used only for research purposes. Of course, the participants had given their permission for this ‘blinded’ testing.
Every PHAROS participant was examined by a neurologist every 9 months for 4 years. This assessment included a number of tests of movement, thinking and behaviour, all of which can be affected in Huntington’s disease.
Most people in PHAROS had CAG repeat counts that were clearly normal (26 or fewer) or expanded (36 or more). But fifty of the participants had CAG counts in the intermediate range.
In a paper just published in the journal Neurology, the PHAROS investigators have reported what they found in these fifty people with intermediate gene.
As expected, the ‘intermediate’ group looked like those with ‘normal’ CAG repeat counts in measures of movement, thinking and day-to-day functioning. That chimes with the current thinking that intermediate CAG repeats don’t cause HD symptoms.
Subtle differences?
However, on one set of tests, the PHAROS team found some unexpected differences. These were ‘behavioral’ measures that ask questions about things like mood, motivation, irritability, aggression and suicidal thoughts. These are areas of brain functioning that are often disturbed in Huntington’s disease.
The behavioral measures in PHAROS revealed that people with an intermediate number of CAG repeats had lower levels of motivation, and reported more suicidal thoughts than those with a normal number of CAG repeats. Other aspects of behavior were not significantly altered, and over a 4 year period there was no worsening of these symptoms.
These differences were found by comparing everyone with an intermediate CAG length against everyone with normal CAG counts. Within both groups there was a lot of variation.
In the Neurology article, the PHAROS researchers suggest that these subtly altered behavioral changes might mean that the brains of people with intermediate CAG counts have some features in common with the brains of people with a fully-expanded huntingtin gene. They raise the possibility that the behavioral differences might even represent very early symptoms of HD.
What does this mean?
The finding that low motivation and increased suicidal thoughts are more common in people with an intermediate CAG count – even when those people don’t know their test results – is certainly an interesting one, because it suggests that the slightly-longer-than normal gene might be causing subtle changes in the functioning of the brain. And if one of those changes is increased suicidal thoughts, then people with intermediate genes might need to be supported more closely than people whose HD test result is definitively negative.
But do these subtle changes represent a very early stage of Huntington’s disease? That’s a very bold claim, and not one that can be proved either way at the moment.
If intermediate CAG repeats could cause HD, we would expect that people with a CAG counts towards the higher end of the intermediate range would show more behavioral problems, but this was not found in the PHAROS study.
Other possible explanations
Another thing to bear in mind is that sometimes, interesting results like this can occur by chance. If you toss a coin ten times, you might get five or six heads in a row, but that doesn’t mean the coin is abnormal. It’s the same with science – the more things you measure, the higher the chance that you’ll find something that appears abnormal.
In the PHAROS study, the researchers looked at eleven different aspects of behavior, as well as many tests of movement, thinking and functioning, but only found ‘statistically significant’ differences in two behavioral measures in people with intermediate CAG counts. It’s possible that those two differences arose through random chance. It’s certainly difficult to explain how people with an intermediate gene might have an increase in suicidal thoughts but didn’t have significantly lower mood scores than people with normal-length genes.
The final thing to remind ourselves here is that this report deals with a small number of people with intermediate CAG lengths, among a large group overall. That makes it possible that one or two people with serious problems might skew the results for the whole group, even if their problems were unrelated to having an intermediate CAG repeat.
Can this research help practically?
Currently, people found to have an intermediate CAG are advised they are not at risk of developing Huntington’s disease and do not usually receive ongoing medical care. That is still our understanding, but new results raise the possibility that they might be prone to these subtle behavioural problems.
Given their findings, the researchers involved in this study suggest that people with an intermediate number of CAG repeats should receive closer monitoring, and treatment if these symptoms develop. That seems like sensible advice. Meanwhile, ongoing research into the full spectrum of CAG lengths will help us figure out whether the problems flagged up here are really caused by intermediate CAG repeat count.


