
Huntington’s disease therapeutics conference 2023 – Day 3
Check out research updates from Day 3 of the 2022 HD Therapeutics Conference #HDTC2023


Welcome to the third and final day of HD science, live from Dubrovnik, Croatia!
Our Twitter updates are compiled below. Continue to follow live updates for the final day of the conference with the hashtag #HDTC2023. Check out our coverage of Day 1 here: https://en.hdbuzz.net/343 and day 2 here: https://en.hdbuzz.net/344.
Biomarkers
This morning’s session will focus on biomarkers, things we can measure to get a picture of a person’s health or their response to a drug. Different types of biomarker measurements might focus on predicting onset, monitoring a person’s HD, or checking drug safety. As we heard last night, NfL levels can help us get a better picture of brain health, but there are other proteins also being studied for this purpose.
HD Clarity
First up is Dr. Niels Henning Skotte from the University of Copenhagen who will be telling us about his work studying biomarkers from HD patient samples. He uses samples from a large spinal fluid collection study called HDClarity https://hdclarity.net/. Niels is first talking about the importance of “quality control” in the spinal fluid samples – tests they do to ensure that they are uncontaminated and properly stored. He also presented some statistics to show how many are needed to answer different types of questions about HD. Many of the proteins which are potential biomarkers are only present in tiny amounts in patient samples.
There are special graphs called “volcano plots” that allow researchers to see which proteins found in spinal fluid differ the most between people with and without the HD gene. Some of the potential biomarkers even show differences between gene-negative and pre-symptomatic gene carriers, which could be helpful in the hunt for treatments that could be administered before symptom onset. When certain protein levels differ between people with and without HD in both blood and spinal fluid, researchers look more closely at them to understand how, and possibly why, their levels shift at different stages of HD. When a protein change is consistent across many people, then it may be considered as a useful biomarker of HD. The role of different proteins in the body is considered, and how they interact with one another, which can give us clues about biological processes affected in HD.
In this age of artificial intelligence or AI, scientists can feed large datasets to computer systems and ask them to consider complex sets of factors to determine which proteins would make the best biomarkers. Niels is using machine learning approaches to do just this. In the future, measuring changes across groups of many proteins prior to the development of symptoms might be used to better track exactly where a person is in disease progression or to decide when they should begin an HD treatment.
Fat molecules as a biomarker for HD
The next speaker is Dr. William Griffiths from Swansea University who will be telling us about how cholesterol and other fat molecules could be used as possible biomarkers for HD. William reminds us that about 25% of the body’s cholesterol is in the brain, and a lot of this is made on site. Some types are able to exit the brain, so we might be able to measure their levels to gain an understanding of brain health. Disruption of the cholesterol-making process and changes in levels of cholesterol have been observed in HD, and in fact there are drug development efforts focused on correcting these changes.
William’s work focuses on measuring the differences between cholesterol levels in people with HD and without HD to see if these molecules could be used as a biomarker. Measuring and analyzing cholesterols requires fancy biochemistry techniques. The specific molecules they are looking for are hard to detect even with top end equipment available, so they had to tweak the system using a cool technique called “click chemistry”. This boosts the signal of the cholesterol from grass-size to tree-size, as William explains. William’s group has found that one form of cholesterol, which is only generated in neurons, is diminished in blood samples from HD patients, making it a potential biomarker.
Somatic instability as a biomarker of HD
Up now is Dr. Darren Monckton from the University of Glasgow who will be telling us about his group’s research on whether some aspects of somatic instability could be a biomarker of HD.
Scientists can measure the levels of somatic instability of the CAG repeat part of the HD gene in all types of different patient samples. Darren uses fancy sequencing techniques to do this as accurately as possible in the DNA from blood donated by people with HD. The Monckton group has mapped out how the expansion of CAG repeats over time (somatic instability) changes at different rates in blood samples depending on the age of the person and their original CAG number.
They have also looked at blood samples from the same individual collected 7 years apart. This gives clues about how somatic instability increases in each person over time. Even over this huge timeframe, the changes are generally very subtle and happen slowly. Being able to measure these small changes is very important, because potential drugs which will alter the rate of somatic instability will also likely have very subtle effects.
These techniques will probably prove to be very useful in some of the clinical trials in the pipeline. HD is not the only disease that has somatic instability, and the techniques in development by the Monckton lab for measuring subtle DNA changes over time will be useful to apply to the study of other genetic diseases and corresponding treatments outside the field of HD.
Tracking Huntington with PET tracing
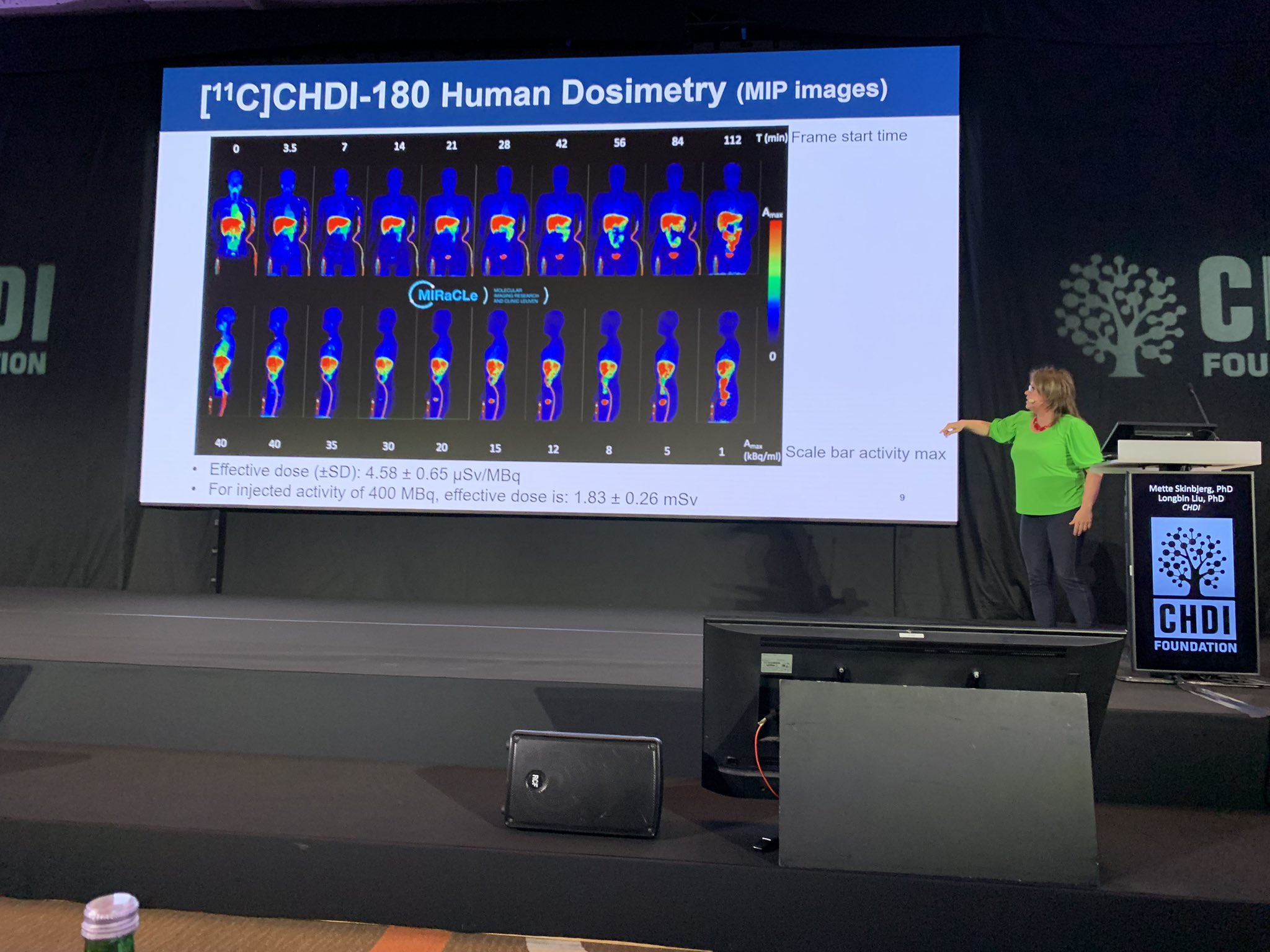
We are back from our coffee break and now we will be hearing from Dr. Mette Skinbjerg about a huntingtin PET tracer which allows tracking of the toxic clumps of protein in the brain which accumulate over time. We wrote about this previously here. Without a tracer, the only way we can see how huntingtin protein accumulates in the human brain is to look at samples after someone has died. Tracers are a safe way to look in living people and could be a great way to see how drugs might be working.
CHDI has been working with academic partners to make a tracer for HD which they have extensively characterised in many different HD animal models including mice and monkeys which allows tracking of the build up of protein clumps over time. Now they are moving beyond the animal models to test their tracer in people. Tracers are labelled with radioactivity so scientists can measure where they stick to the target – in this case the clumps. It’s important tracers leave the body after dosing so exposure to radioactivity is in the safe range.
Although the tracer seems to be safe to use in people, unfortunately the signal in the brain didn’t track with what the scientists expected. This is disappointing but this program taught us a lot about making a tracer for HD which can be used for making better ones in the future. Now the team is working on a new generation of tracers which they are hoping will perform much better. Things are progressing forward in the lab with lots of testing in HD animals so hopefully this next round will work better.
Biomarkers and machine learning
The next speaker is Dr. Peter Wijeratne from the University of Sussex. Peter’s group aims to use biomarkers and machine learning to characterise and predict HD progression in individuals. Very cool!
As researchers continue to identify all sorts of different biomarkers from biofluids, imaging, etc, many biomarkers for one person could be combined for better predictions. But combining and understanding all of this data together is hard for people to do, this is where AI can help us out!
Peter used a fun ChatGPT example to explain machine learning – an algorithm that can adapt and make inferences from patterns in data. He showed how quickly these systems can learn new information and make informed decisions – very cool! To “train” the AI system, you need lots and lots of high quality training data where scientists already know the answers. The AI system can then learn to spot patterns in this data, enabling it to spot similar and related patterns in test data where the answers aren’t known yet.
Peter’s group are looking at brain imaging data from three different studies which looked at how different brain structures change in HD over time. Training AI on these complex and rich datasets, they hope that they will be able to make robust predictions of disease. Turns out, good predictions for disease onset could be made, and the results agreed well with the HD-ISS staging system. They hope this will prove useful for making predictions at the individual level in the future.
HTT levels and tominersen
In the next talk, Dr. Blair Leavitt, a clinician/researcher from the University of British Columbia, will speak about his study of samples from the GEN-EXTEND trial of tominersen. He is diving deeper into how huntingtin levels change with tominersen treatment.
Blair starts by thanking HD family members who so generously and selflessly share biological samples with scientists to create a biobank resource. This is invaluable to scientists to understand HD and how drugs may change the path of this disease. Blair is focusing on one individual in particular, who felt very strongly about donating his brain when he passed. A rich data set and many samples are available from the tominersen trials he participated in, along with his brain tissue, which offers a rare window into drug effects.
Looking at the brain, scientists on Blair’s team were able to measure levels of the drug in different regions and compare this to the exposure levels predicted by earlier monkey experiments. Generally these showed the predictions were pretty good. Next they looked at huntingtin levels in different regions of the brain and how these compare with control brains. As expected for a huntingtin-lowering treatment, the levels in this individual were much lower than in controls. Disappointingly, the levels of huntingtin in the spinal fluid were too low to be quantified for this individual. This means we don’t know how well the brain and spinal fluid levels of huntingtin correlate, for this trial participant at least.
It’s hard to overstate how precious this tissue is for scientists to be able to truly examine in depth how a treatment has affected the brain. Collaborators in the audience will ask additional questions using this tissue so generously donated by this one trial participant.
Clinical trials
After a lunch break, we are back for the last scientific session of the #HDTC2023 conference. This afternoon’s session will be focused on clinical trials, and we’ll be hearing about study design and progress in human research.
Classifying HD stages
Dr. Jeff Long of the University of Iowa is speaking about the HD-ISS, a staging system for HD. It’s a clinical research tool that allows researchers to better classify people in the early stages of HD for more efficient trial design and recruitment.
Now that this new tool is in wider use, Jeff’s team is developing a database of information from large observational trials, like IMAGE-HD, PREDICT-HD, TRACK-HD, and ENROLL-HD, to better understand the timecourse of progression through HD-ISS stages. Having built these tools, Jeff’s team is working to understand how they’d be useful in a clinical trial – how many HD patients at a particular disease stage would be needed to generate robust findings to convince us whether or not a drug worked.
Since the HD-ISS incorporates data from brain images, biomarkers, and genetics, many variables can be considered to define which clinical measurements are the best ones to use to show whether a new drug might be working. Using observational trial databases, researchers like Jeff can apply statistical techniques to better predict how many participants and what types of assessments are likely to be needed to show the benefit of a drug. This is complex and important math that illustrates the importance of participation in observational research.
The proof is in the pudding (or the data)
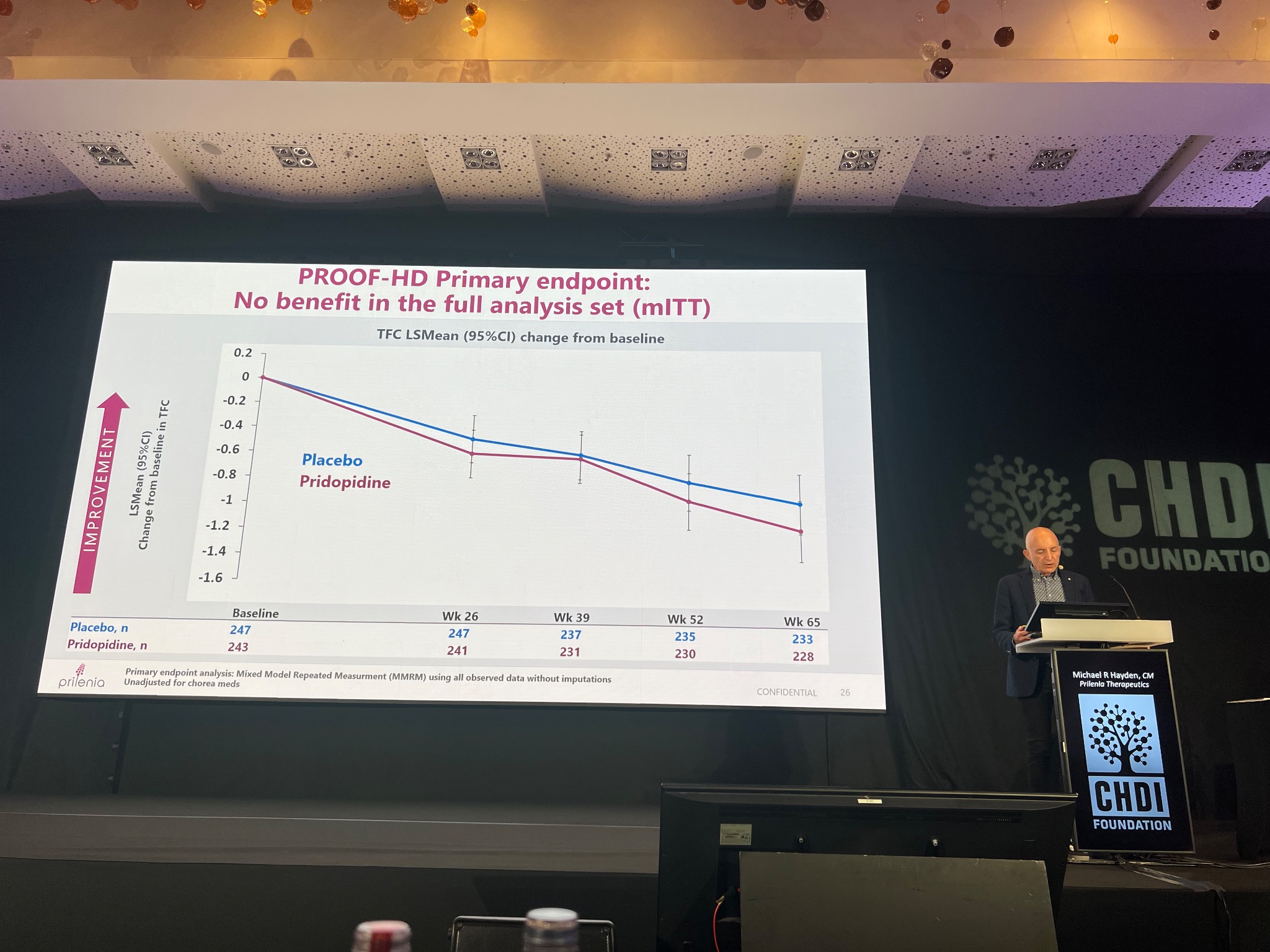
The next talk is a highly anticipated one sharing the very early results of the PROOF-HD Trial of Pridopidine. We learned from press on Tuesday that the trial did not meet its primary endpoints, but now we are seeing the data.
Dr. Michael Hayden, the CEO of Prilenia, is giving this presentation. He is first explaining the mechanism of how the drug is believed to affect nerve cells, in particular its action on a type of receptor that facilitates communication between neurons, known as sigma 1.
The PROOF-HD trial was designed to use certain clinical assessments, a combination of movement, behavior, and thinking tests, to see if pridopidine helped slow the worsening of HD symptoms over the course of about a year and a half. Trials are designed with “primary,” “secondary,” and “exploratory” endpoints. Showing that a drug affects primary endpoints is usually how decisions are made to continue developing the drug and eventually to get it approved. This trial recruited fast, and most participants stayed in it the entire time, a testament to the mobilization and commitment of HD patients. When the vast majority of people continue in a long trial, it can also speak to the safety and tolerability of the drug.
The main overall finding is that the trial’s primary endpoints were not met. In this case it was a measurement of people’s ability to function day-to-day. On average, people taking pridopidine and people taking placebo functioned similarly for the duration of the trial. Another important endpoint was a combination of different movement, behavioral, and thinking measures, and these also did not improve for people taking pridopidine. Pridopidine might have shown some benefits in one movement measurement, called the Q-motor, but this was not statistically significant.
When a trial is designed, but before it begins, the sponsor (in this case Prilenia) has to make decisions about what types of statistics and analyses it will perform once the results are in. In PROOF-HD, Prilenia decided they would separate groups of participants into those taking drugs called neuroleptics (also known as neuropsychotics) and those not taking neuroleptics. This is because pridopidine affects some of the same biological pathways as neuroleptics. When Prilenia looked at data just from people who weren’t taking neuroleptic drugs, the potential benefit was more obvious using some clinical measurements, especially in the first year. Ultimately this also was not statistically significant.
Michael is now showing data from a trial of pridopidine in people with ALS, a disease which has some shared biology with HD. This trial also showed some potential benefits on secondary outcomes.
Prilenia believes that there remains some promise for pridopidine for treating HD, and the company will now focus on delving deeper into the data. They especially need to understand how different neuroleptic treatments affect response to the drug.
Red light for branaplam
Up next, Dr. Beth Borowsky, of Novartis, describes the results of their trial with a drug called branaplam in HD patients. We wrote about this drug and its surprising mechanism of action here.
While branaplam was safe in children with another disease (spinal muscular atrophy), some animal studies had indicated there was a possibility of damage in the nerves that project from the brain to the skin and muscles of the body. Based on that concern, Novartis included specialized experts in that kind of nerve damage amongst treated HD patients, just in case such a symptom emerged during the trial.
Unfortunately, over a few weeks, some subtle movement and lab measurements started to suggest that the feared risks had actually emerged. In consultation with their independent expert safety monitors, Novartis decided to initially pause dosing. At the time of pause the patients had gotten treatment from between 5 and 22 weeks. After careful review, they found that 78% of the treated patients showed one or more signs that could indicate nerve damage, and also some changes in brain structures called ventricles.
Based on a very careful analysis of the benefit and the risk for patients, Novartis made the decision to halt the trial in December 2022. We covered this here. Currently, all the participants in the trial are continuing to be monitored for symptoms of nerve damage and to track how that may change over time after they stopped taking the drug.
Beth has brought a snapshot of data that Novartis collected to bring the HD community up to speed on what they found. First – as hoped, branaplam lowered Huntingtin levels by around 25% in the spinal fluid, suggesting that branaplam was able to lower levels of Huntingtin in the brain.
Unfortunately, Novartis also found higher levels of a protein called neurofilament light, or NfL, a marker of unhappy brain cells. We’ve talked about NfL before, since it increases in the normal course of HD, and it was a big focus of the biomarkers session at this meeting. We’d hope that if an HD drug works, levels of NfL will go down over time. But in the branaplam study, Novartis discovered that NfL levels in the blood and spinal fluid increased with treatment. This is one of the findings that helped encourage Novartis to pause the study.
In parallel to these lab tests, physicians were carrying out careful nerve function studies in each participant. About 86% of participants had some kind of neurological symptom, and brain imaging showed larger fluid-filled cavities known as lateral ventricles.
All together, it seems like Novartis’s drug did what they thought it would do – reduce Huntingtin levels in the brain. Unfortunately, this was accompanied by serious side effects, so there is not a safe path forward for this drug. Importantly, Novartis is continuing to monitor the trial participants and to analyze data to inform drug development moving forward.
AMT-130 marches forward
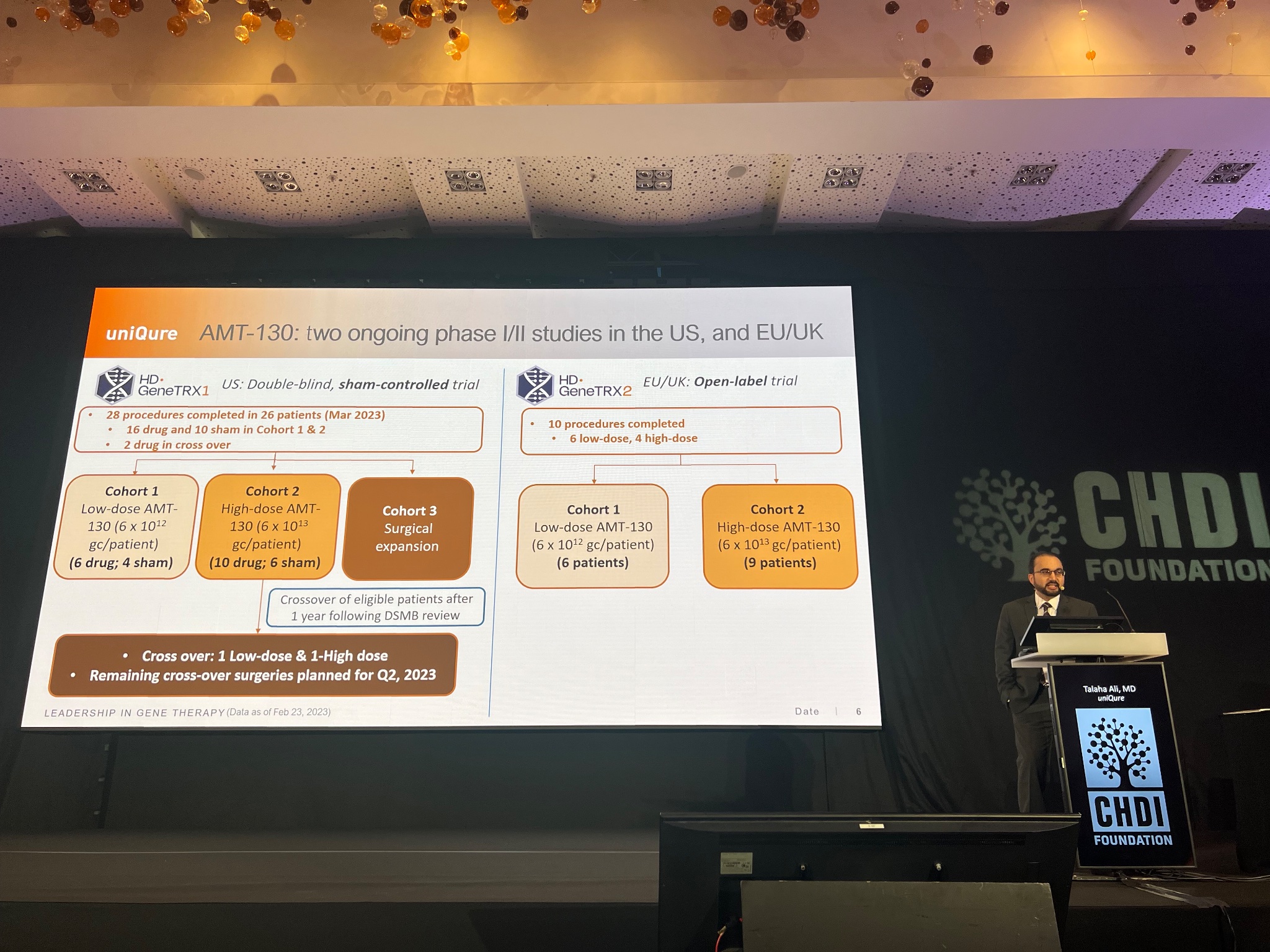
Up next, Dr. Talaha Ali from uniQure is giving an update on their study of an HD gene therapy for HD called AMT-130. This relies on the injection of harmless viruses that carry instructions to teach brain cells how to reduce HTT levels.
The amazing thing about these viral gene therapies is that they theoretically require only a single injection, as the viruses persist in the brain for many years – perhaps forever. The downside of this is that it requires surgery to deliver the viruses into the brain. This surgical approach is being tested in two separate trials – one in the US and one in Europe. Because this is such cutting edge stuff, only small numbers of people are being included – around 40 patients in total.
Patients in the trial receive very careful, very slow, injection of the drug into different parts of the deep brain structures that are most impacted in HD. The trial is testing a low dose and a high dose of AMT-130, and closely monitoring participants for the first year and then more frequently for up to 5 years. uniQure will be sharing new data and updates soon, likely by the end of June 2023.
As previously covered, along the way uniQure had some concerning reactions in three patients. After careful examination, the independent doctors monitoring these symptoms decided that the risk seemed acceptable, and the trial was continued.
Excitingly, uniQure has some evidence that AMT-130 reduces brain levels of Huntingtin in the CSF – but to date, the number of treated patients is much too small to make accurate estimates. Hopefully more exciting data to come next time we hear from uniQure!
Narrowing the targets for tominersen
The next talk is by Dr. Peter McColgan from Roche, which is developing a drug called tominersen for HD. He’ll talk about the history of the program, what they’re learning from tominersen trials, and what’s happening with the ongoing GENERATION HD2 trial.
Ionis originally developed tominersen, a spinally delivered genetic drug called an ASO. In early, short safety trials, it was the first drug able to lower huntingtin levels in humans. This was followed by a very large trial to test effects on HD symptoms, known as GENERATION HD1. We learned in March of 2021 that GENERATION HD1 had been halted because of safety concerns – tominersen wasn’t helping HD patients, and at the highest dose it may even have been hurting.
Later, Roche dived deeper into the data, and found that some participants in GENERATION HD1 may have benefitted from tominersen, specifically those who started the trial at a younger age and with less severe symptoms. For this reason, Roche designed and launched the GENERATION HD2 trial, which is a smaller study testing tominersen in a younger population of people in the earliest stages of HD. This study is recruiting now and eventually there will be up to 75 sites in 15 countries.
Peter is now showing data on NfL, a protein that can serve as a marker of damage to nerve cells. New analyses of data from GENERATION HD1 show that giving tominersen at lower doses is likely safer based on lower levels of NfL. The GENERATION HD2 trial is testing two different, lower levels of tominersen, and mathematical modeling predicts that these lower doses will be safer because they will not lead to such large increases in NfL.
Now Peter is sharing new NfL data from the GENERATION HD1 trial. Towards the end of the trial, it actually looks as though NfL levels are going down with tominersen, which is further evidence that the lower doses being tested in GENERATION HD2 could have some promise.
Here’s Peter’s whole presentation on tominersen.
That concludes the research talks at the 2023 HD Therapeutics Conference. Thanks for following along, and visit http://hdbuzz.net to read summaries of Day 1, Day 2, and Day 3!
For more information about our disclosure policy see our FAQ…


