Uncovering the dark side of DNA repair to design HD treatments
A gene called MSH3 helps to repair our DNA, but in HD it can slip up and cause CAG repeats to lengthen. Researchers have uncovered new information about how MSH3 activity is controlled, opening the door to new therapeutic avenues.
By Emma Bunting December 22, 2020 Edited by Dr Leora Fox and Dr Rachel Harding
A gene known as ‘MSH3’, which encodes a protein involved in fixing and maintaining our DNA, has become a hot topic in Huntington’s research since being implicated as a key driver of the disease by multiple genetic studies. In a recent publication, a team of scientists from the National University of Ireland, Galway, have provided insights as to how the MSH3 protein is controlled within our cells, which could help to inform the design of drugs aimed at slowing or even preventing HD.
MSH3 – the double-edged sword
The MSH3 protein molecule works by correcting genetic mistakes and protecting our genomes against the continuous onslaught of DNA damage that they face on a day-to-day basis. It does this by scanning along our DNA, looking for errors and recruiting other proteins to help fix them in a process called ‘mismatch repair’.
As you may know, Huntington’s disease is caused by an unusually long stretch of repeating ‘C’-‘A’-‘G’ DNA bases (the building blocks of the genetic code) within a gene called “huntingtin”. In the brain areas affected by HD, this stretch of repetitive DNA is ‘unstable’ - meaning that more repeat units might be added throughout life. We call this process ‘DNA repeat expansion,’ or somatic instability. For most repeat expansion diseases like HD, the longer the stretch becomes, the worse the disease symptoms get.
When MSH3 comes across this CAG repeat in our DNA, it recognises it as an error and tries to fix it, but instead introduces even more repeats - making matters even worse!
So how can we prevent this?
If we could make a drug that stops MSH3 from making this mistake, we could slow or prevent the repeat expansion process, which in turn we hope could slow down the disease – or even stop it dead in its tracks… But how can we do this without disturbing MSH3’s normal function of protecting our genetic code? Normally, when DNA repair genes are missing, all sorts of problems can arise through the accumulation of DNA damage – like cancer, for example. What’s really exciting about MSH3 is that, unlike other DNA repair proteins that are known to be involved in the repeat expansion process, completely getting rid of MSH3 does not seem to have many negative side effects. It has a great cover system arranged for when it’s not there - making it an ideal druggable target.
So what’s new?
“If we could make a drug that stops MSH3 from making this mistake, we could slow or prevent the repeat expansion process, which in turn we hope could slow down the disease – or even stop it dead in its tracks ”
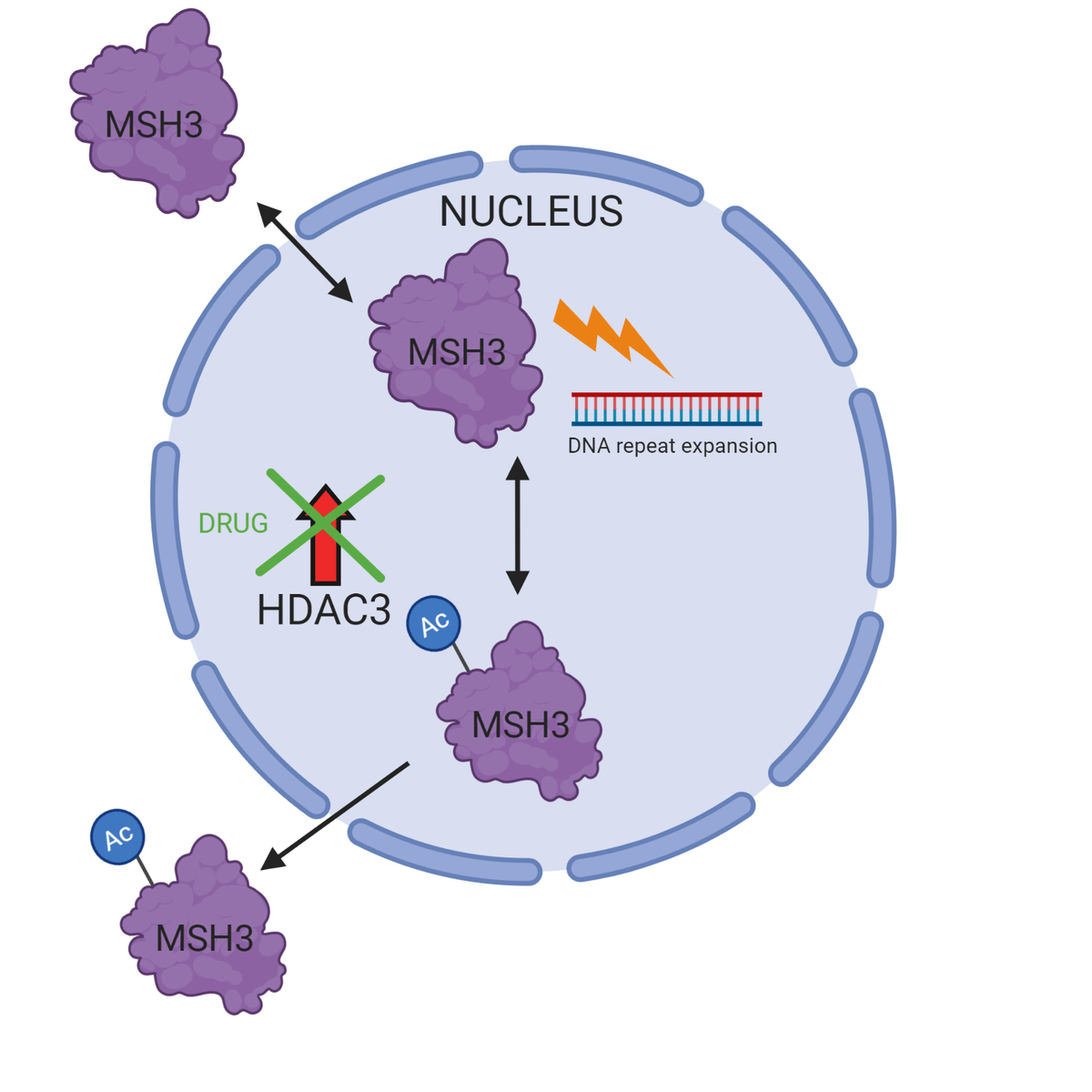
Our cells can make the MSH3 protein work slower by adding a chemical signature called an acetyl group, and can make it work faster by removing the acetyl group. Since MSH3 working faster would mean more rapid DNA repeat expansion, scientists want to prevent the erasure of this acetyl mark. Previous studies suggest a protein called HDAC3 is involved in the removal process. The Laheu lab at the National University of Ireland, Galway, tested a drug in human cells that stops HDAC3 from working properly, and looked at its effect on DNA repeat expansion.
What did they find?
They found that the drug halted CAG repeat expansions in human cells, and, most importantly, they found it did not affect other important DNA repair activities, suggesting this therapy would not come at the cost of increased cancer risk. The researchers also used this drug to understand more about how HDAC3 controls MSH3 activity. Protein molecules have special signals called ‘Nuclear Localisation Sequences’ (or ‘NLS’ for short), which act like a postal code that directs proteins to the nucleus where our DNA is kept. They realised that the acetyl mark alters MSH3’s postal code, directing it out of the nucleus where it can no longer drive DNA repeat expansions.
So what does this all mean?
Overall, their study suggests a new regulatory mechanism for DNA repeat expansions through removal of acetyl groups from MSH3 by HDAC3. This may provide an explanation for why patients with certain versions of MSH3 have slower disease progression, if, for example, their acetyl group is more difficult to remove.
Understanding disease mechanisms in this way opens doors for the design of drugs aimed at slowing down the DNA expansion process (and in turn, the disease itself) – particularly since they claim HDAC3 inhibition does not affect the core function of DNA mismatch repair. The drug they used in this study is powerful, selective and fairly well studied, so may already be a promising clinical candidate in itself.
That said, messing with HDAC’s can have all sorts of other unwanted effects in cells. We would need to make sure drugs targeting HDAC3 are safe with limited side-effects. What’s more, we would need to come up with a way of delivering the HDAC3 inhibitor to the deep regions of the brain that are affected in Huntington’s disease, which tends to be pretty difficult.
In summary, their work shows promise, but much more work needs to be done before we can get excited about this as a potential therapy.


