
The genetic 'gray area' of Huntington's disease: what does it all mean?
Intermediate alleles and reduced penetrance – the genetic 'gray area' of Huntington’s disease, explained
By popular request, a special feature article on the often confusing topic of ‘intermediate allelesintermediate alleles HD genes with CAG lengths between 27-35, which do not result in HD symptoms, but are longer than normal. Intermediate alleles are thought to be at risk of expanding in the offspring of people who carry them.’ and ‘reduced penetrance’ – the genetic ‘gray area’ that frequently comes up in discussions around genetic testing for Huntington’s disease.
Having a genetic test for Huntington’s disease is an extremely worrying time. The only thing you want to hear when you go for the result is whether or not you are going to develop HD. Most people do get a clear answer to this question, but for a small minority, the answer is not quite as simple because they receive a result in the ‘gray’ area known as either a ‘reduced penetrance allelereduced penetrance allele A copy of the huntingtin gene with a CAG-repeat length long enough to cause symptoms in some, but not all, people who carry it.’ or an ‘intermediate alleleintermediate allele A copy of the huntingtin gene with a CAG-repeat length that never leads to disease for the carrier, but may place the carriers children at some risk of HD.’. The meaning of these results can be confusing, but we hope this article will help set things straight.
The Genetic Basics

Genes are made up of the genetic material called DNA. DNA is the code for all life and is made up of a combination of 4 ‘letters’ – A, C, G and T. Scientifically, these genetic letters are called ‘nucleotide basesnucleotide bases A single ‘letter’ of the genetic code, abbreviated A, T, G or C’.
The HD gene provides the code for the huntingtin proteinhuntingtin protein The protein produced by the HD gene., and everyone inherits two copies of the gene – one from each parent. The genetic mutation that causes HD is a long sequence of repeated C-A-G nucleotides in the HD gene.
Scientists love jargon, and sometimes use the term ‘alleleAllele one of the two copies of a gene’ instead of gene; but basically these terms mean the same thing.
The number of CAG repeats in the HD gene determines whether or not someone will develop HD during their lifetime. Everyone has two copies of the HD gene – one from their father and one from their mother. HD testing involves measuring the CAG repeatCAG repeat The stretch of DNA at the beginning of the HD gene, which contains the sequence CAG repeated many times, and is abnormally long in people who will develop HD length in both HD genes of an individual, using DNA obtained from a blood sample.
The number of CAG repeats in an HD gene can range from less than 10 to more than 120. The average number of CAG repeats is around 17. HD is a ‘dominantdominant A genetic condition that only requires one copy of a mutation to occur’ disease, which means that an individual only needs one of their two HD genes to have a larger-than-normal number of CAG repeats for them to develop the disease.
Two facts are quite straightforward:
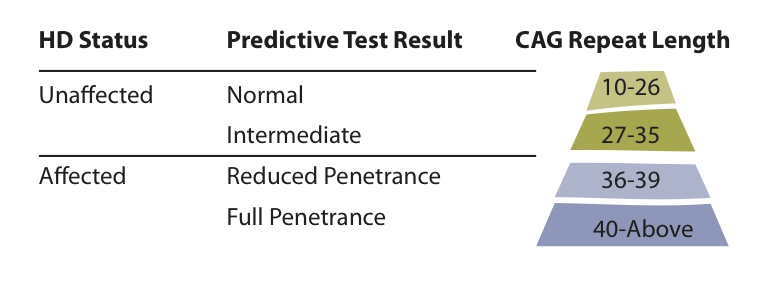
If both copies of a person’s HD gene contain 26 or fewer repeats, they will not develop HD, and nor will any of their children.
and
If one copy of an person’s HD gene has 40 or more repeats, they will develop HD in their lifetime, and each of their children will have a 50% risk of inheriting the expanded HD gene.
An HD gene with 40 or more repeats is called a full penetrance gene. That means the person will definitely develop HD in their life, as long as they don’t die prematurely of another cause.
The ‘Gray area’
The clinical meaning of results becomes more complicated when the HD gene has a repeat length between 27 and 39 CAGs – often described as the ‘gray area’.
People with an HD gene containing between 36 and 39 repeats are in the ‘reduced penetrance’ range. Some people in this range will develop symptoms of the disease, while others won’t.
Unfortunately, it’s impossible to predict which people with a reduced penetrance gene will or won’t develop the disease. If symptoms do occur, they tend to begin later in life and are generally less severe.
Children of an individual with an HD gene in the ‘reduced penetrance’ range are each at 50% risk of inheriting a gene with either ‘reduced’ or ‘full’ penetrance.
‘Intermediate allelesintermediate alleles HD genes with CAG lengths between 27-35, which do not result in HD symptoms, but are longer than normal. Intermediate alleles are thought to be at risk of expanding in the offspring of people who carry them.’, on the other hand, have repeat lengths between 27 and 35 CAGs. People with an intermediate alleleintermediate allele A copy of the huntingtin gene with a CAG-repeat length that never leads to disease for the carrier, but may place the carriers children at some risk of HD. will not develop HD themselves, but there may be a risk of HD developing in their children.
What about Future Generations?
The number of CAG repeats in an HD gene can be unstable when the gene is passed on to the next generation. That means the number of CAG repeats can increase or decrease when the gene is passed from parent to child.
We don’t know for sure why the HD gene is unstable, but we think it has something to do with how accurately DNA is copied by cells. If you were asked to type ‘CAG’ 50 times, you might find that you actually end up typing a couple of extra ‘CAGs’ by accident, or a couple too few. The machinery in cells that copies DNA also makes mistakes when copying long lengths of repetitive DNA.
Changes in repeat length are called ‘expansions’ when more CAG repeats are passed to the next generation, and ‘contractions’ when fewer CAG repeats are passed to the next generation.
The unstable HD gene causes problems when it comes to predicting what will happen to the next generation. Although people with intermediate allelesintermediate alleles HD genes with CAG lengths between 27-35, which do not result in HD symptoms, but are longer than normal. Intermediate alleles are thought to be at risk of expanding in the offspring of people who carry them. (27 to 35 repeats) will never experience HD symptoms themselves, the repeat inherited by their children can be longer than their own. Their children are at risk of inheriting a reduced penetrance or full penetrance gene.
In the same way, someone with a reduced penetrance gene (36 to 39 repeats) can pass on a full penetrance gene to a child, if the gene expands.
A few factors can influence whether expansion occurs. The first is the starting length of the CAG repeatCAG repeat The stretch of DNA at the beginning of the HD gene, which contains the sequence CAG repeated many times, and is abnormally long in people who will develop HD. Normal repeat lengths of 26 or less are stable, and don’t change when passed on. But full penetrance genes – those with repeat lengths of 40 or more – are more likely to expand in the next generation.
Intermediate and reduced penetrance alleles are generally more stable than full penetrance genes, but can still expand, giving rise to longer repeat lengths in the next generation.
Other factors influencing CAG repeatCAG repeat The stretch of DNA at the beginning of the HD gene, which contains the sequence CAG repeated many times, and is abnormally long in people who will develop HD expansion are the sex and age of the parent. Fathers are much more likely than mothers to pass on an HD gene with an expanded number of CAG repeats. However, the sex of the children doesn’t make a difference.
Older fathers are more likely than younger fathers to pass on an expanded copy. This may be because new sperm are made throughout a man’s lifetime, allowing more DNA copying mistakes as the man gets older.
Currently, it’s not possible to estimate the exact risk of CAG repeatCAG repeat The stretch of DNA at the beginning of the HD gene, which contains the sequence CAG repeated many times, and is abnormally long in people who will develop HD expansion, for people with intermediate or reduced penetrance alleles. However, the risk that people with intermediate or reduced penetrance alleles will pass on an expanded alleleAllele one of the two copies of a gene to their children is thought to be small.
The importance of family history.
It’s possible to develop HD even if there are no known family members with the condition. Around 10% of people with HD don’t have a family history.
Sometimes, that’s because a parent or grandparent was wrongly diagnosed with another condition like Parkinson’s disease, when in fact they had HD. Now that we have a reliable genetic test, this doesn’t happen as often as it used to.
In other families, HD appears for the first time because a parent who would have developed HD died from another cause before they started showing symptoms, but had already passed the gene on to their children.
Another way that HD can occur in a family with no previous history is when a new genetic mutation for HD occurs. New mutations come from intermediate allelesintermediate alleles HD genes with CAG lengths between 27-35, which do not result in HD symptoms, but are longer than normal. Intermediate alleles are thought to be at risk of expanding in the offspring of people who carry them.. They happen when a parent with an intermediate alleleintermediate allele A copy of the huntingtin gene with a CAG-repeat length that never leads to disease for the carrier, but may place the carriers children at some risk of HD. (27-35 repeats) passes on an expanded alleleAllele one of the two copies of a gene in the HD range. Later in life, the son or daughter will develop HD, but the parent with an intermediate alleleintermediate allele A copy of the huntingtin gene with a CAG-repeat length that never leads to disease for the carrier, but may place the carriers children at some risk of HD. will remain symptom-free. Intermediate allelesintermediate alleles HD genes with CAG lengths between 27-35, which do not result in HD symptoms, but are longer than normal. Intermediate alleles are thought to be at risk of expanding in the offspring of people who carry them. are often identified in parents whose children have a new HD mutation.
Intermediate allelesintermediate alleles HD genes with CAG lengths between 27-35, which do not result in HD symptoms, but are longer than normal. Intermediate alleles are thought to be at risk of expanding in the offspring of people who carry them. aren’t just found in families where a new mutation has been identified – they can also crop up in families where HD is known about. This happens when someone with an intermediate alleleintermediate allele A copy of the huntingtin gene with a CAG-repeat length that never leads to disease for the carrier, but may place the carriers children at some risk of HD., who’s not from an HD family, has children with someone who has a fully penetrant alleleAllele one of the two copies of a gene.
If one of that couple’s children decides to have HD genetic testing later, they might learn that they didn’t inherit the HD gene from their HD-affected parent, but did inherit an intermediate alleleintermediate allele A copy of the huntingtin gene with a CAG-repeat length that never leads to disease for the carrier, but may place the carriers children at some risk of HD. from the other parent. Families are often surprised to learn that there is an intermediate alleleintermediate allele A copy of the huntingtin gene with a CAG-repeat length that never leads to disease for the carrier, but may place the carriers children at some risk of HD. on the non-HD side – but in fact, this is the most common way intermediate allelesintermediate alleles HD genes with CAG lengths between 27-35, which do not result in HD symptoms, but are longer than normal. Intermediate alleles are thought to be at risk of expanding in the offspring of people who carry them. for HD are identified.
It’s not currently possible to estimate the exact risk that someone with an intermediate or reduced penetrance allelereduced penetrance allele A copy of the huntingtin gene with a CAG-repeat length long enough to cause symptoms in some, but not all, people who carry it. will pass an expanded alleleAllele one of the two copies of a gene to their children. The risk is small, but further research in this area is underway.
Summary
A small number of people having a test for HD will have a result which falls into the ‘gray area’ area of intermediate allelesintermediate alleles HD genes with CAG lengths between 27-35, which do not result in HD symptoms, but are longer than normal. Intermediate alleles are thought to be at risk of expanding in the offspring of people who carry them. and reduced penetrance.
Someone with an intermediate alleleintermediate allele A copy of the huntingtin gene with a CAG-repeat length that never leads to disease for the carrier, but may place the carriers children at some risk of HD. (27-35 CAG repeats) will not develop HD. Their children have a low risk of inheriting a gene with an increased number of CAG repeats, in either the reduced or full penetrance range.
Someone with a reduced penetrance allelereduced penetrance allele A copy of the huntingtin gene with a CAG-repeat length long enough to cause symptoms in some, but not all, people who carry it. (36-39) may or may not develop HD in their lifetime. Their children are at a 50% risk of inheriting an HD gene with either reduced or full penetrance.
Intermediate and reduced penetrance alleles mean that predictive test results are not always black or white. Researchers are working to understand these ‘gray area’ genes better, so we are better able to prepare people for testing and explain results to patients and their families.
Acknowledgements
HDBuzz thanks Alicia Semaka for her expert advice about intermediate alleleintermediate allele A copy of the huntingtin gene with a CAG-repeat length that never leads to disease for the carrier, but may place the carriers children at some risk of HD. risk. Alicia is a genetic counsellor at the Centre for Molecular Medicine and Therapeuticstherapeutics treatments, University of British Columbia, who studies genetic risk in HD.
Learn more
For more information about our disclosure policy see our FAQ…


