
Huntington's disease therapeutics conference 2021 – Day 3
Catch up on all of the latest updates from day 3 of the 2021 CHDI Huntington’s disease therapeutics conference #HDTC2021



We are back for the last day of the virtual 2021 CHDI Therapeutics conference. This article summarises our live Twitter updates on the exciting science being presented, which you can find with the hashtag #HDTC2021. The final session of the conference will provide the latest news on more Huntington’s disease clinical programs.
A new way to define the different stages of HD
The first talk of the day was from Sarah Tabrizi and Jeff Long who presented the HD Integrated Staging System (HD-ISS), which aims to redefine the different stages of HD to encompass all the complexities and variability of HD progression.
The new system is a result of lots of hard work by the HD Regulatory Science consortium, a global network of academics, industry scientists and experts in drug regulation. The HD-RSC exists to put in place a framework that lets good drugs for HD get tested and approved smoothly.
The main aim of HD-ISS is to enable clinical trials to include people before they develop movement problems from HD (motor diagnosis). These trials would aim to prevent or delay HD onset. Tabrizi pointed out that the HD-ISS framework is not a reinvention of clinical diagnostic or staging criteria – it is purely a research tool to allow selection and monitoring of patients for clinical trials – an important distinction.
Current trials use staging systems based on “landmarks” with cutoff values. The most obvious in HD is the concept of “motor diagnosis” which is what was used to diagnose HD even before we knew the genetic cause. But biologically, we now know HD is a continuum – it develops slowly, affects people very differently, and has a long period where people feel and look normal, but we can show with things like blood tests and scans that the mutation has had some effect on the brain.
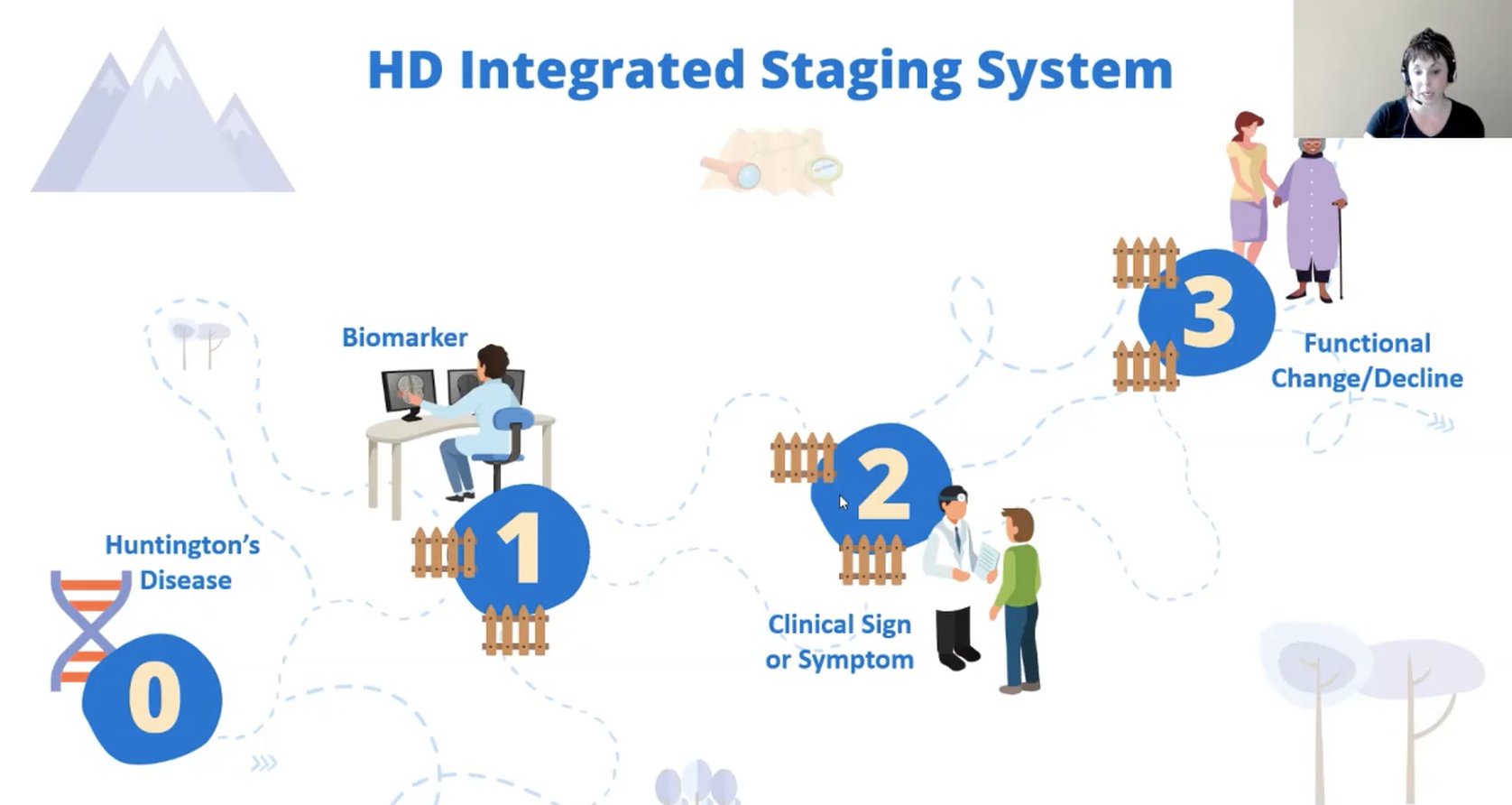
For research purposes, Tabrizi proposes a new definition of HD. She conceptualises HD as 4 changes happening in a sequence: The disease (the lifelong effect of the gene); being able to detect the gene’s effects (biomarkers); symptoms; and functional change (loss of ability to do stuff).
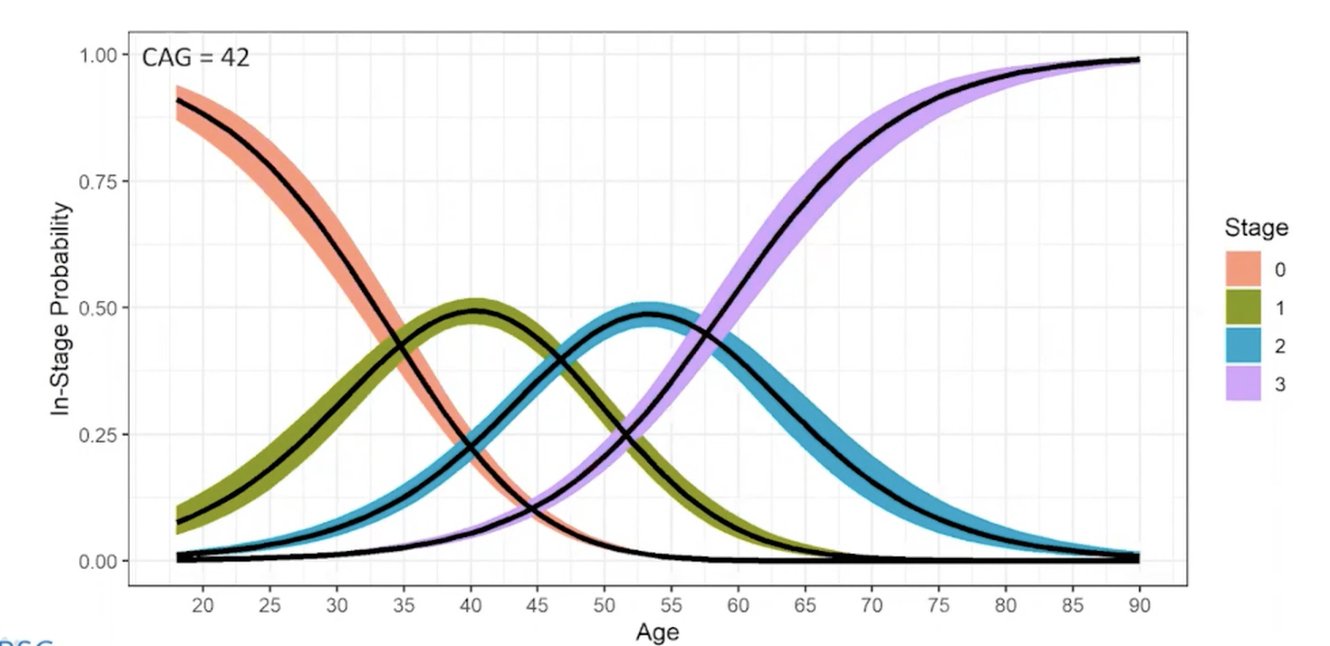
These changes are expressed as stages 0 to 3 and the transition from one stage to another is defined by agreed landmarks. Jeff Long explained that the cutoff values for each landmark were determined systematically from large datasets, for example, monitoring the volume of the caudate lobe of the brain as measured by MRI. Crunching the numbers lets Long plot trajectories showing how a person might be expected to move through the stages during their lifetime.
Tabrizi explained that this kind of modelling lets drug developers plan trials because terminology will be unified including the possibility of intervening before motor symptoms emerge. Importantly, HD-RSC sought input from non-scientist HD family members via the HD-COPE network.
Updates on the huntingtin-lowering trial HD-GeneTRX1 from uniQure
The next speaker was David Cooper who gave updates on the uniQure huntingtin-lowering gene therapy trial, testing the drug AMT-130 which we recently wrote about.
AMT-130 is the first gene therapy for HD. It is packaged inside a harmless virus and delivered to the brain via a one-time surgery. Once there it acts to inactivate the recipe for huntingtin protein. Cooper told us about how AMT-130 was tested in large and small animals and was shown to be safe and well distributed to important regions of the brain.
Next, Cooper introduced the Phase I/II study, called HD-GeneTRX1. It involves 26 people who will get one of two dose levels of AMT-130, or will undergo an imitation surgery. They will be followed closely for a year and more infrequently for up to 5 years. This is a safety study so the main objective is to make sure patients do not experience any dangerous side effects.
Participants are between 25-65 and have early HD symptoms. They also need to have a CAG repeat of 44 or more, and to meet other criteria regarding the size of certain brain areas so that the procedure can be performed safely. The criteria evolved a bit as they screened patients and learned from the first surgeries.
10 patients have now been treated by brain surgery which is performed in an MRI. This is cutting-edge science and has provided valuable lessons learned to the neuroscience community thanks to the selfless volunteers in this study. There are nine sites recruiting patients in the USA and uniQure will be starting a small study in Europe later this year, in which everyone will receive the drug (known as an open-label trial).
In the Q&A, Cooper was asked whether the Roche trial results changed uniQure’s plans for this trial. He explained that right now they are moving forward as planned, and that their surgical delivery method is different from that used by Roche.
Diving back into the data from the SIGNAL trial
The final speaker of the session was Maurice Zauderer from Vaccinex. Zauderer presented results from the recent SIGNAL trial which looked at whether the drug pepinemab helped HD symptoms. We previously wrote about this here.
In this study, around 250 people with early HD symptoms received pepinemab for over a year via a monthly IV injection, and they were monitored for safety and whether it could help with symptoms. The focus was on measuring and observing serious side effects, cognitive and movement symptoms. The drug was safe but they saw no overall improvement in patients in different cognitive tests which assess planning and memory.
When Zauderer and colleagues teased out the data, they do see some small benefits of treatment in a subset of patients who are showing early signs of symptoms but this was not the case in a patient subset not showing symptoms.
The SIGNAL trial did not meet its primary endpoint and these findings have arisen from a subsequent analysis of the trial data. Although this benefit in people with HD symptoms with early signs of disease is potentially good news, this would need further study.
Towards a more collaborative HD research community
The final speaker of the conference was Aled Edwards of the Structural Genomics Consortium, who spoke about how the HD scientific community and in particular industry researchers might better collaborate at the level of drug discovery, the process of identifying genes and pathways to target with therapeutics. Drug discovery often starts with a huge array of possibilities that get narrowed down over time as research reveals more about the biology of HD.
Edwards is a huge proponent of open science and data sharing, and he suggested that the perceived legal and financial barriers to doing this, even within the private sector, can be easily overcome and could benefit individuals with HD and many other diseases. The HD community is already so tightly collaborative that it could potentially set the bar for others by implementing some of these strategies. Excellent food for thought at the end of three packed days of sharing the latest in HD research amongst academics, clinicians, and members of industry.
Looking forward to HDTC 2022 already!
And that’s all folks! We hope this has been a helpful way for everyone to learn about all of the latest news in the pursuit of medicines to treat HD.
For more information about our disclosure policy see our FAQ…


