Fresh Updates from First Huntingtin Lowering Study Publication
Hot off the presses – New publication gives more details about the results of Ionis and Roche's safety study with a Huntingtin-lowering ASO

Today saw the publication of the first manuscript describing a huntingtin lowering trial in Huntington’s disease patients. This study, sponsored by Ionis and Roche, provided clear evidence of researchers’ ability to safely reduce mutant huntingtin protein in the spinal fluid. An overview of these results has previously been shared, but this manuscript provides important new information about the results of this remarkable trial. What’d we learn?
Huntingtin lowering: a little background
Huntington’s disease (HD) is caused by a single mutation in a gene we refer to as the HD gene. Like most genes, the HD gene is used by cells as instructions to create a little cellular machine called a protein, which we call huntingtin. The genetic mutation that causes HD also changes this protein, which we refer to as mutant huntingtin.
While HD symptoms are complex, it has pretty simple genetics – if you inherit a single mutant copy of the HD gene from either your mother or father, you will develop HD. Since we know that one has to inherit a mutant HD gene to develop HD symptoms, could we interfere with the process of making the mutant huntingtin protein? If so, would that slow or prevent the progression of Huntington’s disease?
That general approach, which we refer to as huntingtin lowering has been a major focus of HD researchers for a number of years, and several companies are pursuing this target. Two companies – Ionis and Roche Pharma – are running the most advanced program, in collaboration with a number of academic researchers around the world led by Prof. Sarah Tabrizi, University College London.
We’ve previously discussed the early results of the first human study by Ionis and Roche here, subsequently updated here and here.
Excitingly, today saw the release of the first official manuscript describing these huntingtin lowering efforts in HD patients, and it provides new information about the first trail. This trial was focused on understanding whether treatment with a huntingtin lowering drug called an antisense oligonucleotide or ASO is safe.
Endpoints, Endpoints, Endpoints
As in any clinical trial, this study included a number of endpoints. Endpoints are just the target, or goal, that you want your study to accomplish. In future HD trials, this might include things like improved movement or thinking. But for a new drug that has never been tested in people, the endpoint is always safety, safety, safety.
Formally, researchers say that safety is the primary endpoint of the study. This just means it’s the sole criteria we’ll use to judge whether the trial is a success or failure. If the drug turns out to be unsafe, the trial fails. If there are no safety concerns, the study is a success.
While we’d obviously like be able to tell whether a drug is safe and whether it helps HD symptoms at the same time, we can’t achieve both goals in the course of a single study. This is because it takes large numbers of participants – many hundreds – to tell whether a drug is influencing HD symptoms. But for a safety study, we want to treat the smallest reasonable number of people to reduce the number of people exposed to the risk of testing a drug for the first time.
While trials usually have one primary endpoint, researchers are curious about other possible impacts of their drug on HD-related changes. These other measurements are called secondary endpoints – this term helps us remember that the main, or primary, goal of the trial is to determine safety, but we have many secondary measurements we’re interested in examining.
This study included a large number of secondary endpoints, focused on participants’ HD symptoms, brain scans and lab tests to measure specific markers in the blood and spinal fluid. The new manuscript is exciting, because it’s the first chance we’ve had to look at the raw data produced in the study. The interesting results of some secondary endpoints are discussed below, but it’s important to remember that determining safety was the primary goal of everyone working on this trial.
No Serious Adverse Events
“Since we know that one has to inherit a mutant HD gene to develop HD symptoms, could we interfere with the process of making the mutant huntingtin protein? If so, would that slow or prevent the progression of Huntington’s disease?”
The data published in this new paper generally supports the safety of the drug, called Htt-Rx, in HD patients. The most important safety outcome measure is a list of what researchers call adverse events. These can be anything that causes distress to people, running the gamut from mild (a headache that resolves in a few days without treatment) to severe (a heart attack or suicide attempt).
Of course, in any group of dozens of people followed closely for several months, there’s bound to be some adverse events. This is why having a placebo, or dummy treatment, group is so important in studies like this. By comparing the rate at which people in the trial experience adverse events, we can measure whether they occur more frequently in people given real drug, as opposed to the placebo injections.
There were no severe adverse reactions in any of the groups in the trial. Excitingly, no participants withdrew from the study, suggesting folks in the trial felt able to handle the repeated spinal injections and many tests administered.
Mild adverse events did occur during the study, but people receiving placebo treatment were exactly as likely to experience them as people receiving the drug. This suggests that these effects are not due to the drug itself, but rather the procedure of spinal fluid injections, or just bad luck. The most common side effect was a post-treatment headache, which is known to occur sometimes after spinal fluid injections.
NfL Changes
This study used several newly developed tests that raise some potential safety concerns worthy of additional study. First, the team measured the levels of a marker called neurofilament light, or NfL, in the spinal fluid of people in the study. This marker is released by sick and damaged brain cells called neurons, and researchers have previously demonstrated that it increases slowly and predictably in HD mutation carriers (covered on HDBuzz here).
Surprisingly, in the patients receiving higher doses of ASO, there was a brief increase in the levels of NfL, suggesting some kind of stress on neurons after delivery of a high dose of drug. According to the data presented in the paper, this increase in NfL returned to normal during the course of the study, even though people continued to receive injections of the drug. The meaning of this isn’t clear – researchers were measuring NfL in hopes of eventually seeing a reduction in its levels, not an increase. However, the increase was relatively small, and seems to have returned to normal.
This increase in spinal fluid NfL is weird, frankly, and you can be sure that researchers at Roche are thinking about how to get to the bottom of it in the longer, on-going, studies with this drug. If there were any sign that this increase in NfL levels was associated with adverse impacts on brain function, we would know by now, so that doesn’t seem to be the case.
Brain Imaging Changes
Another finding worthy of additional study arises from brain imaging called magnetic resonance imaging or MRI. This kind of brain scan uses giant magnets to take a picture of the shape of participants’ brains. Many years of work by HD researchers have defined very precise changes in brain shape that occur as HD progresses. One of these changes is a progressive increase in the size of the brain’s ventricles – the fluid filled spaces within the brain tissue. During the course of HD, these spaces appear to grow, as the tissue around them shrinks.
In the higher-dose groups, the volume of these fluid-filled spaces actually increased during the study, which is the opposite effect one would hope for if the drug was slowing brain shrinkage. This effect could be a real response to ASO treatment, or it could be due to unexpected physical changes in the brain thanks to some other aspect of delivering large doses of ASOs, and have nothing to do with HD.
As with the brief increases in NfL, the impact of these brain changes is not yet clear. What is clear is that these changes aren’t associated with changes in brain function, at least as far as researchers can tell in this initial study.
Getting to the bottom of these potentially concerning lab tests requires a larger group of people, followed for a longer time. This is exactly why Roche and Ionis are conducting a new, larger, study called the GENERATION-HD1 study, the announcement of which we covered on HDBuzz here.
Where do ASOs go?
Another major outcome from this study is a better understanding of how ASOs move around the body after being injected into the spinal fluid. Based on a large number of animal studies, Ionis and Roche built a computer program to predict how much ASOs would be found in the spinal fluid (and brain) after being injected into people.
Models like this are really important because they help researchers plan how much drug to inject, and how frequently they need to inject it to keep levels of the drug high enough to do its job. In the study of HTT-Rx, researchers measured how much ASO was in the spinal fluid (and blood, where it shows up as it’s being cleared away).
These results proved that the computer program was accurate at predicting how much ASO sticks around in the spinal fluid. This gives us confidence that the amount of ASO being injected, and the frequency at which it’s being injected, are based on good assumptions. This will reduce the amount of guesswork involved in planning the next trials with this drug.
mHTT Knockdown
The overall goal of all this work is to reduce levels of mutant huntingtin in the brain. Unfortunately, for now, there’s no direct way to measure mutant huntingtin in the brains of living patients. Brain tissue is irreplaceable, so we can’t sample it to determine how much mutant huntingtin is there.
Luckily, we can guess at this by measuring levels of mutant huntingtin in the spinal fluid. This clear liquid bathes the brain, circulating and coming into contact with our entire brain throughout the course of a day.
For reasons that are still a little bit unclear, a tiny amount of mutant huntingtin is present in the spinal fluid of HD patients. Our current best guess is that this mutant huntingtin comes from the brain itself, rather than some other source. So, researchers have developed very sensitive tests for measuring mutant huntingin levels in spinal fluid, to give a clue about the levels of mutant huntingtin in the brain.
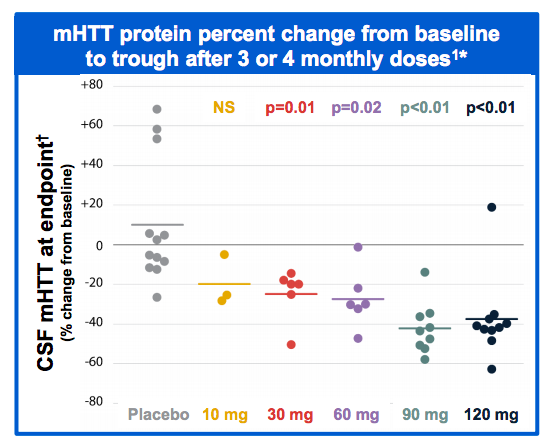
Treatment with ASOs resulted in very clear reductions in levels of mutant huntingtin in the spinal fluid. While it’s not direct proof of lowering huntingtin in the brain, it’s the best evidence we could hope for to suggest that the drug has successfully lowered huntingtin levels.
“Treatment with ASOs resulted in very clear reductions in levels of mutant huntingtin in the spinal fluid. ”
What about HD symptoms?
Finally, investigators examined the relationship between treatment with Htt-Rx and HD symptoms. Remember, the duration and number of people in this study is intentionally low, to minimize the risk associated with testing a drug in people for the first time. That means there’s not enough people in the study – and they weren’t followed long enough – to be definitive about any changes seen in symptoms. And, indeed, there is no large difference in the HD symptoms measured in participants during this short study.
Thanks to newly developed lab tests for measuring mutant huntingtin in the spinal fluid, we have a sense of how much mutant huntingtin lowering is occurring in each patient. As an early exploration of their data, the researchers examined the relationship between how much mutant huntingtin was lowered in the spinal fluid of each participant, and the severity of their HD symptoms.
There are some intriguing correlations observed – notably, people with the greatest reduction in mutant huntingtin tended to also have better symptoms. The researchers appropriately point out that these results should be taken with a grain of salt until we look in a bigger group of people for a longer time, but it’s very exciting that larger reductions of mutant huntingtin are correlated with better HD symptoms.
Take Home Message
The study described in this new manuscript represents a huge investment of time, effort and hope by everyone involved. The 46 volunteers and their families deserve enormous gratitude from the HD community, as they took on some risk in testing a drug with the potential to address HD’s underlying cause. Physicians and researchers in academic labs, at Roche and especially at Ionis also deserve enormous credit for developing these drugs and bringing them to patients for testing.
What did we learn as a result of all this hard work? First – that lowering mutant huntingtin in the nervous system of HD patients is possible. This represents the first time we’ve been able to lower levels of the protein that causes HD in a targeted way. Second, we learned an enormous amount about how ASOs work in the body – how long they stick around in the spinal fluid and blood, which helps design future studies with more targeted delivery of drugs.
The primary endpoint of the trial, to determine whether this drug is safe, was met. There were no severe adverse events associated with this ASO being delivered to the spinal fluid of HD patients. There were some lab tests – including NfL and brain ventricle size – that do raise some questions that need to be addressed in future studies. Luckily, these lab test results weren’t associated with changes in brain function that we can measure.
In short, the now published results of the first study with a drug targeting the root cause of HD are a big leap forward for the community. They point towards refinements and cautions we should consider as we test the drug in larger groups of HD patients over a longer time. In fact, the next studies with this drug are already underway, suggesting everyone involved is working towards the goal of determining as quickly as possible whether these drugs are both safe and effective against HD.
For more information about our disclosure policy see our FAQ…


