
Melatonin treatment success in HD mice
Melatonin delays disease onset and extends survival in Huntington's disease mice – could it do the same for patients?

Melatonin, a hormone produced by the pineal gland in the brain, is available in pill form and used to treat sleeping disorders. New research suggests that it can slow down Huntington’s disease in model mice – great news, but it doesn’t mean everyone should rush to take it.
Melatonin and the pineal gland
Melatonin is a hormone – a signaling molecule produced by the body and released into the bloodstream.
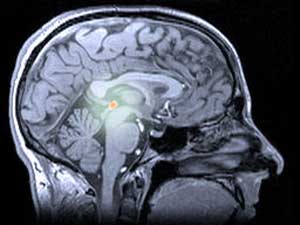
In humans and other animals, melatonin is produced by the pineal gland (pronounced ‘pie-kneel’), a slightly mysterious structure deep within the brain. The pineal gland is sometimes referred to as a ‘third eye’, because in some lizards, it’s located on the top of the head, and is used to detect the shadows of flying predators.
Light and dark are also important for the human pineal gland, and the melatonin it produces. The pineal gland receives light signals from the eyes, and releases melatonin when it’s dark. The melatonin acts on the brain’s sleep centers and makes us drowsy. In the longer term, the daily fall and nightly rise in melatonin regulates our pattern of sleeping and waking, keeping it in sync with changes in daylight.
How does melatonin work?
The short answer is that we don’t really know. Like most hormones, melatonin is released and whizzes round in the blood, until it meets a ‘receptor’ molecule on the surface of a cell. Melatonin has two types of receptor – called MT1 and MT2. When melatonin binds to a receptor, a series of chemical reactions inside the cell are triggered, ultimately causing subtle changes in the activation of different genes. It’s probably those gene activation changes that govern the effects of melatonin on sleep.
Beyond sleep
Melatonin keeps surprising scientists, though. Unlike many hormones, melatonin has potentially important chemical properties beyond its ability to activate MT1 and MT2 receptors. It’s an antioxidant, which means it can ‘mop up’ harmful chemicals produced when cells release energy from food.
Because of these properties, it’s been suggested that melatonin may have effects that go way beyond the regulation of sleep – including possibly beneficial effects on things like memory function and cancer. The evidence for these effects is unclear, though.
Melatonin as a drug
Melatonin is available in pill form. In the USA and Canada, it can be purchased over the counter, while in Europe it’s only available on prescription. It’s taken at bedtime to help sleeping, and is quite popular with shift workers and jet-setting travelers.
The amount of melatonin produced by the pineal gland falls slowly as we age, so in some countries melatonin is only approved for use in the elderly.
Not all melatonin pills are the same. The doses vary quite a bit, and some are ‘prolonged release’, meaning the melatonin is released gradually rather than rapidly. Prolonged release melatonin tablets, taken at bedtime, mimic the natural pattern of melatonin more closely.
Melatonin in Huntington’s disease
Some people with Huntington’s disease take melatonin already, and it’s gaining popularity among HD doctors. Sleep problems, especially a disturbed pattern of sleeping and waking, are common in HD. Studies have shown that HD patients produce less melatonin at night than people of the same age who don’t have HD. This may be one reason why people with HD can have problems sleeping, that can sometimes be helped by taking melatonin in the evening.
Disease-modifying and symptomatic treatments
‘Disease modification’ is the holy grail for Huntington’s disease researchers. A disease-modifying drug is one that reduces the damage caused to cells by the HD genetic mutation, preventing or slowing symptoms.
“Melatonin-treated mice retained their movement control for several weeks longer, and survived around 20% longer”
At present, melatonin is used as a ‘symptomatic’ treatment – that’s one that improves symptoms like disturbed sleep, without an expectation that it will prevent HD from getting gradually worse.
There are lots of symptomatic treatments for different aspects of HD, which can make a huge difference to people with the disease. Effective symptomatic treatments are better than nothing – but what we really want is disease-modifying treatments. If we’re really lucky, some disease-modifying treatments might turn out to be good for symptom control, too.
Might melatonin be disease-modifying?
In 2008, a group of researchers led by Dr Robert Friedlander of the University of Pittsburgh, USA, wondered whether any drugs that were already on the market might be able to protect neurons against harm. They tested over a thousand drugs, and melatonin was one of only two that seemed to work.
Our cells have mechanisms for dealing with harmful situations. First, they have ‘stress responses’ that can protect them against dangers like excessive heat. When things get really tough, and a cell is damaged beyond repair, it can sacrifice itself in a controlled way, to prevent damage to nearby cells. Scientists call this noble act ‘programmed cell death’, or ‘apoptosis’ (pronounced ‘a-pop-TOE-sis’).
In their 2008 work, Friedlander’s team gave melatonin to cells with the HD mutation, grown in a dish. The cells lived longer, and had fewer chemical signs of programmed cell death. This was an early suggestion of a possible disease-modifying effect of melatonin in HD.
What’s new?
Since 2008, Friedlander has been trying to figure out how melatonin protects cells with the HD mutation. A new publication in The Journal of Neuroscience sets out the progress that’s been made.
Through a number of different experiments, Friedlander’s team showed that melatonin treatment produced a number of different effects in cells grown in the lab. Melatonin-treated cells had less active programmed cell death systems, more stable electrical activity and more effective garbage removal. Any of these might be helpful.
Friedlander wondered whether these effects were produced by melatonin attaching to its MT1 or MT2 receptors – or whether they might be direct chemical effects because of the anti-oxidant properties of melatonin.
When the cells were instructed not to produce the MT1 receptor, the protective effects of melatonin were lost. That suggests that melatonin attaching to MT1 is the important step. Getting rid of the MT2 receptor didn’t alter the effect of melatonin, confirming that MT1 is the more important receptor.
Curiously, Friedlander found that cells with the HD mutation actually had fewer MT1 receptors on their surface, especially when they were stressed. That might make it harder for cells to receive the protective effect of melatonin when they need it most. Thankfully, one effect of melatonin treatment was to restore the number of MT1 receptors.
Melatonin treatment in HD mice
The next step was to test melatonin in an animal model of HD. Friedlander chose an HD mouse model called the R6/2 mouse. R6/2 mice become unwell rapidly, so they’re useful for testing drugs quickly. They usually die within 6 months of birth, whereas a normal mouse can live several years.
From a young age, half the mice were given melatonin every day by injection, while half received dummy injections. The mice receiving melatonin retained their movement control for several weeks longer, experienced less brain shrinkage, and survived longer too – around 20% longer, in fact. And several chemical markers of cell death were reduced in the melatonin-treated mice.

Melatonin treatment didn’t reverse all the effects of the HD mutation – the mice still lost weight, died prematurely, and still accumulated blobs of mutant huntingtin protein in their neurons.
What about humans?
Friedlander’s team concluded their work by looking at the melatonin signaling system in brains donated by HD patients after they died – a precious gift to the HD community.
They found reduced levels of the MT1 receptor – like what they’d seen in the cells with the HD mutation. This doesn’t prove that melatonin would be effective in humans, but suggests the changes in the cells are echoed in the human brain.
Should I be taking melatonin?
Through careful research, Freidlander’s team have put together a solid case for the beneficial effects of melatonin in cells with the Huntington’s disease mutation. And a 20% increase in life expectancy, together with delaying of symptoms, in an HD mouse, are encouraging results.
It’s still early days for melatonin as a disease-modifying drug, though. It would be premature to conclude that HD-affected people should take melatonin to prevent or slow the disease.
Melatonin isn’t the first drug that’s been shown to improve the R6/2 mouse – in fact, dozens of drugs have done it before. But so far, each one that’s been tested in human patients has failed to show the same benefit. The R6/2 mouse is just much easier to treat than human patients.
Trials in humans are expensive to run properly, and each one carries risk for the participants. For this reason, many HD researchers feel that drugs should be tested in several different model animals to choose the best ones to take forward into human trials.
Of course, melatonin has the advantage of being approved for human use, indicating that it’s already been through important safety trials. Crucially, though, that doesn’t guarantee that it’s safe or effective for slowing HD.
Another drug that worked well in HD mice – minocycline – was recently shown to be ineffective in HD patients. Alarmingly, when tested in motor neuron disease (ALS), minocycline actually made things worse. That kind of unexpected result is why it’s so important to test drugs properly in controlled trials.
So, melatonin needs to be studied further in animals, and a trial in human patients may be the next step.
Meanwhile, melatonin is already in use as a treatment for the sleep symptoms of Huntington’s disease. There are several sleep-enhancing drugs to choose from, and these results for melatonin in HD mice might be one factor to consider when deciding what drug to try.
Learn more
Sources & References
For more information about our disclosure policy see our FAQ…


